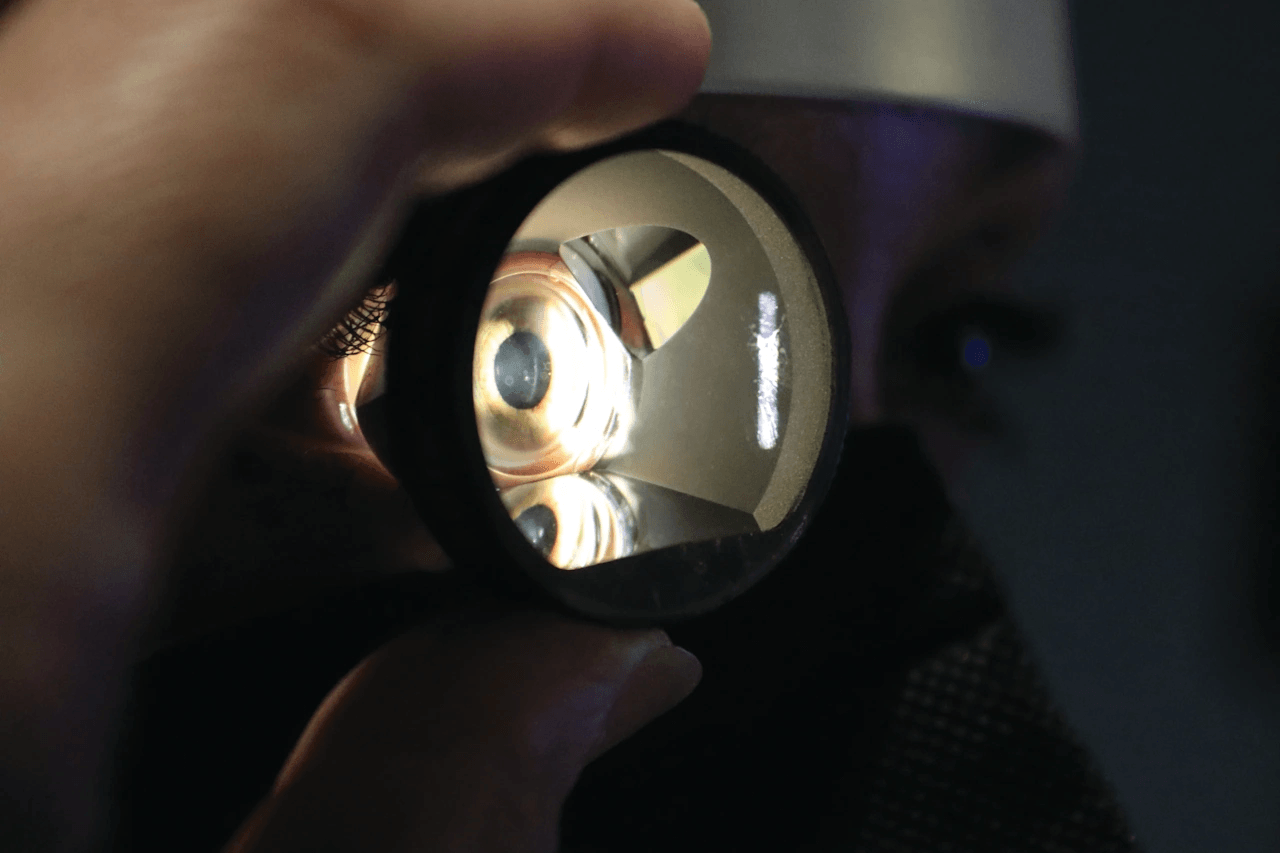
A gonioscopy lens is one of the least expensive instruments in an eye-care practice and one of the few that imaging still cannot replace. It is also the one most often bought by brand name out of habit, when the decision really comes down to two things: whether the lens views the angle directly or through mirrors, and how those mirrors are arranged. Get those right and a five-minute exam catches a narrow angle before it blinds someone. Get them wrong and you have bought a lens that slows the exam
Toggle Nav

News
-
- June 30, 2026 - 11 min read
-
- June 30, 2026 - 11 min read
A fetal Doppler does one job: it makes the fetal heartbeat audible. The same two words, though, cover two very different products. One is a consumer gadget sold for a few dollars to expectant parents who want to listen at home. The other is a clinical instrument a midwife, obstetrician, or family physician relies on at every prenatal visit. They look similar. They are not the same purchase, and a clinic that buys the wrong one finds out quickly.
This guide is for the clinical buyer: practice managers,
-
- June 30, 2026 - 10 min read
An EMT jump bag is a portable inventory of decisions made in advance. When a crew arrives on scene, there is no time to wish a tourniquet had been packed or that the oxygen tank had been checked. The bag has to already hold the right items, in the right sizes, in working order. That is why a contents checklist organized by clinical function, rather than a random pile of supplies, is the foundation of a reliable response.
This checklist is organized the way care actually unfolds: airway, breathing,
-
- June 12, 2026 - 7 min read
Quick answer: To size an exam glove, measure the circumference of your dominant hand around the knuckles, excluding the thumb, in inches, then match that number to the manufacturer's sizing chart (an 8-inch measurement is roughly a size 8 or medium). A properly fitting glove is snug but not restrictive, with fingertips aligned and little extra material. Sizing is not standardized across brands, so always check the specific manufacturer's chart, and choose the material and fit to match the task.
In
-
- June 12, 2026 - 7 min read
Quick answer: For most medical and clinical settings, nitrile is the best all-around exam glove: it offers strong puncture and chemical resistance, good durability, and is latex-free, so it avoids allergy risk. Choose latex when you need maximum dexterity and tactile sensitivity and latex allergy is not a concern. Choose vinyl for low-risk, short-duration tasks where cost and frequent glove changes matter most. The wrong match shows up as tearing, poor tactility, allergy reactions, or wasted money.
-
- June 11, 2026 - 8 min read
Quick answer: The reliable way to identify a surgical instrument is to read its anatomy rather than memorize appearances. Every ringed instrument shares the same parts, tips, jaws, box lock, shank, ratchet, and ring handles, and the details of each part reveal the instrument's identity and use. A ratchet means it locks closed (a clamp or needle holder); serrated jaws grip tissue; toothed tips grasp tough tissue; smooth tips are atraumatic. Reading these features lets you name an instrument and tell
-
- June 11, 2026 - 7 min read
Quick answer: There is no fixed number of surgical instruments. Estimates range from well over 10,000 distinct instruments in worldwide use to more than 100,000 variations in global production, and the number keeps growing. The reason there is no single count is that one instrument type spawns dozens of variations across sizes, specialties, and designs. What makes the vast number manageable is classification: by function (six core categories), by specialty, and by reusable versus disposable.
"How
-
- June 10, 2026 - 8 min read
Quick answer: Medical equipment pricing is negotiable. The most effective approach: get a fully itemized quote so you can see every line, gather competing quotes from at least three suppliers to establish leverage, bundle or consolidate orders to increase your volume, and negotiate the total value of the deal (warranty, service, delivery, payment terms) rather than only the unit price. Use refurbished offers as a benchmark, build long-term supplier relationships, and put every agreed term in writing.
-
- June 10, 2026 - 8 min read
Quick answer: Group purchasing organizations (GPOs) pool many buyers' volume to negotiate discounts, typically saving practices 5 to 25% and reducing administrative work, with membership usually free. They save the most on commodity supplies and for smaller buyers with little leverage. But GPO prices are not automatically the lowest; a federal study found they were sometimes higher than direct-negotiated prices. The best strategy is to use a GPO as your baseline and negotiate directly where your
-
- June 09, 2026 - 9 min read
Quick answer: Equipping a new ambulatory surgery center typically costs $500,000 to over $5 million depending on operating room count and specialty, with a single-specialty two-OR center commonly running $500,000 to $1.5 million. Buy room by room (pre-op, OR, PACU, sterile processing), standardize equipment across rooms, build around surgeon preference cards, use a GPO or direct negotiation for leverage, and use refurbished equipment for the high-ticket capital items where it cuts cost most without
Recent Posts
-
Gonioscopy Lens Buying Guide: Direct, Indirect, and the Mirrors That Matter
 June 30, 2026
June 30, 2026 -
Fetal Doppler Guide: Clinical vs Over-the-Counter Use
 June 30, 2026
June 30, 2026 -
Eye Occluder Buying Guide: Solid Occlusion vs the Pinhole Test
 June 30, 2026
June 30, 2026 -
EMT Bag Contents Checklist: What to Stock, by Category
 June 30, 2026
June 30, 2026 -
Exam Glove Sizing and Selection Guide for Healthcare Settings
 June 12, 2026
June 12, 2026